Question & Answer - Oral Sensory-Motor, Myofunctional, Vocal Tract, & Airway Information
What is Orofacial Myofunctional Therapy? - Part 1June 2015 |
|||
|
Answer from Barbara J. Greene, Orofacial Myofunctional Therapist and Instructor, living in Santa Barbara, CA Orofacial myofunctional therapy (sometimes referred to as tongue thrust therapy) has existed since the 1400’s with varying degrees of acceptance and practice. Orofacial myofunctional disorders (OMDs) include specific conditions or behaviors that can have a negative impact on oral postures and functions. The common denominator for orofacial myofunctional conditions is a change in the inter-dental arch vertical rest posture dimension called the freeway space. The purpose of orofacial myofunctional therapy (OMT) is to: -Eliminate poor oral habit patterns (such as thumb-sucking, nail-biting, and other biting/sucking habits); -Normalize the freeway space; -Improve cosmesis with a lips-together rest posture; -Achieve nasal breathing; -Establish normal function of the tongue at rest and during the swallow; -Create a normal and harmonious oral-facial muscle environment; and -Restore equilibrium to the mouth, face, head, neck, and body by changing function and behaviors. An easier way to think of it is, “We teach you to chew, breathe, and swallow a new way.” In the drawings of the face and mouth below, you will begin to see the relationship between normal function and dysfunction. Recognizing the symptoms of dysfunction becomes easy because they surround you daily in yourself, your family, your friends, and your co-workers; on the movie screen and TV; and in the general populace. Unfortunately, the dysfunction is frequently not correctly diagnosed, and referrals are often not made. Instead, only the symptoms are treated, vast sums of money are spent, and the patient pays the price for the lack of a correct diagnosis. Corrective orofacial myofunctional therapy is effective, does not involve a long period of treatment, and has a dramatic effect on the rest of a person’s life.
An open-mouth posture often causes several adverse effects: -The eyes have a droopy, sleepy appearance; -There is a tendency to see more “whites” of the eyes in the lower portions of the eyes; -The nasal-sinus area becomes flat in what is called a “long face syndrome;” -The nose becomes smaller, and frequently congestion/allergic reactions are present; -The upper lip becomes shorter and the lower lip becomes fuller; and -The palate shape is affected becoming narrow and/or vaulted which may cause bite deformities. Genetics, of course, also play a role in facial appearance. The goal of orofacial myofunctional therapy is to create normal function and a more stress-free looking face.
In an incorrect resting tongue posture, the tip of the tongue is against either the lower or upper anterior teeth or between them and the rest of the tongue is low within the mouth. Frequently, the lateral borders of the tongue are flared between the teeth. You will notice that without the tongue resting across the top of the mouth, the palate becomes high and narrow and the nasal airway becomes small and compromised. Even though the swallow itself has a certain amount of force, the rest position of the tongue is probably more important than the swallow itself because the tongue exerts a continuous pressure within the mouth at rest over long periods of time during a 24-hour period.
In a dysfunctional swallow, there is insufficient backward pull of the tongue (allowing air to be swallowed). Even though the back of the tongue may be pulling up toward the palate, the middle of the tongue loses contact with the palate, and the tip of the tongue is forward against or between the teeth. Frequently the lateral borders of the tongue flare out to contact the cheeks. The dysfunctional swallow can be unilateral with the flare just to one side, bilateral with the flare to both sides, anterior with the pressure against or between the teeth, or any combination of these. The chin and lip muscles tighten to help facilitate the gathering of saliva instead of the posterior muscles of the face and tongue participating in the swallowing process. Some symptoms of a dysfunctional orofacial muscle environment may be: -Sucking of the thumb, fingers, or tongue; -Biting and sucking habits of the nails, lips, cheeks, tongue, and/or objects such as clothing or hair; -Lips apart posture when the mouth is at rest and/or mouth breathing; -Long face syndrome; -Allergic rhinitis, and frequent colds or illness; -Poor head-neck-body posture; -Stressed facial muscles; -An overdeveloped chin/mentalis muscle; -Many poor facial mannerisms; -Sleep disorders; -Jaw joint pain and/or sounds (i.e., temporomandibular joint dysfunction -TMD); -Headaches; -Neck and shoulder tension; -Ear ringing, called tinnitus; -Bruxing and jaw clenching; -Asymmetry of the perioral muscles; -Periodontal/gum disease and tooth loss; -Speech problems and mumbling; -Enlarged tonsils and adenoids; -Tongue, lip, and/or buccal ties; -Orthodontic/surgical difficulty; and/or -Reflux, gas, burping, hiccups, and/or stomach aches. Correction of orofacial myofunctional disorders is achieved with daily exercises, 2 - 3 times per day for 10 - 20 minutes each over a 3 - 6 month period, followed by an observation phase of 6 - 8 months. Generally, all of the above mentioned symptoms disappear by providing stability to the orofacial muscle complex via orofacial myofunctional therapy. About the Author Barbara J. Greene is an orofacial myofunctional therapist and instructor who has been in practice since 1971. She has a website http://www.tonguethrust.com/ where people can learn about Barbara’s evolution as an orofacial myofunctional therapist and the services she offers, as well as visit her learning center which contains informative articles, videos, and links. Follow this link to contact Barbara. Permissions Permission to print this article was granted by Barbara J. Greene. The drawings and photos are also the property of Barbara J. Greene, and she has granted permission for the printing of these. |
|||
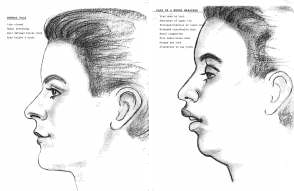 In a normal face, the chin, nose, and lips are in alignment; there are nice facial contours; the eyes are bright; the nose is open for adequate air; and the head-neck-body posture is in alignment. With incorrect facial structure, open lip posture causes the chin to drop down and back. As a result, it is like a weight hanging from the chin causing a downward pull and an inward push of the facial muscles.
In a normal face, the chin, nose, and lips are in alignment; there are nice facial contours; the eyes are bright; the nose is open for adequate air; and the head-neck-body posture is in alignment. With incorrect facial structure, open lip posture causes the chin to drop down and back. As a result, it is like a weight hanging from the chin causing a downward pull and an inward push of the facial muscles.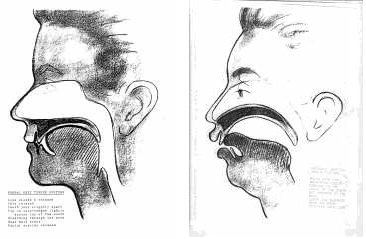 A correct resting tongue posture is how our tongue should be 24-hours a day whenever we are not talking, laughing, eating, drinking, yawning, or coughing. The tip of the tongue is ¼ inch behind the upper anterior teeth with the rest of the tongue resting against the palate and the sides of the tongue contained within the teeth.
A correct resting tongue posture is how our tongue should be 24-hours a day whenever we are not talking, laughing, eating, drinking, yawning, or coughing. The tip of the tongue is ¼ inch behind the upper anterior teeth with the rest of the tongue resting against the palate and the sides of the tongue contained within the teeth.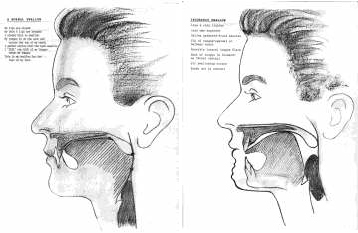 In a correct swallow, the tip of the tongue is ¼ inch behind the upper anterior teeth, the tongue is across the top of the mouth, and the back of the tongue is pulled back making contact with the back of the palate. The uvula and soft palate are pulled up and back. The chin and lips are relaxed.
In a correct swallow, the tip of the tongue is ¼ inch behind the upper anterior teeth, the tongue is across the top of the mouth, and the back of the tongue is pulled back making contact with the back of the palate. The uvula and soft palate are pulled up and back. The chin and lips are relaxed.